
Published on
Updated
A feat of nature, the hand is a wonderful tool that accompanies us on a daily basis to grasp, touch, feel, manipulate… Exploration of the anatomy of the hand with Professor Bertrand Coulet, Head of the Hand and Limb Surgery Department Superior Paralysis Surgery at CHU Lapeyronie in Montpellier.
The hand, by its constitution, its ability to move, its mobility, is exposed to the dangers of daily life. How to explore its anatomy? What are the pathologies that can hinder the functioning of the hand and how to treat them?
The anatomy of the hand
The hand consists of two parts: fine hand consisting of the thumb and index finger for fine grips. And the hand for power take-offs, that is to say the long fingers which allow to have a grip. These two sectors have a different innervation. The median nerve will innervate the fine hand, the motricity of the intrinsic and extrinsic muscles of the thumb but also of the index finger as well as their sensitivity. The ulnar nerve innervates the powerful muscles of the flexors of the 3rd, 4th and 5th fingers which have an overall contraction for the grips between the fingers and the palm (grip). The dominant hand, the one with the most strength, corresponds to the hand that is solicited the most.
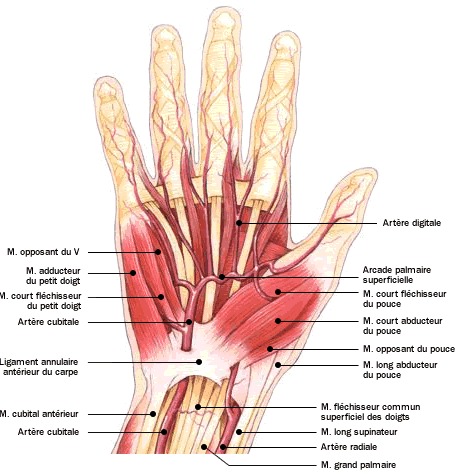
Anatomically, the hand is made up of bones (carpals, metacarpals), phalanges (14 phalanges with three phalanges per finger except for the thumb which has only two), ligaments, muscles (thenar eminence, hypothenar eminence), tendons (tendons that circulate in the hands are the termination of extrinsic muscles that are located in the forearm, and intrinsic muscles located in the hand itself / flexor tendons of the fingers and wrist on the anterior face of the wrist, extensor tendons of the fingers and wrist dorsally), arteries (radial artery externally and ulnar artery internally), veins and nerves (median, radial, ulnar). All these elements connected to each other endow the hand with extraordinary mobility.
The hand is attached to the arm via the wrist. It is able to perform three main axes of movement: flexion-extension of the wrist, lateral inclination and rotation.
The hand allows grasping but also exploration, which at the same time exposes it to trauma, vulnerating agents, toxic substances. “It is probably the segment of the musculoskeletal system with the greatest concentration of noble structures”, says Professor Bertrand Coulet, Head of the Hand and Upper Limb Surgery Service for Paralysis at CHU Lapeyronie in Montpellier. “The slightest wound, the slightest trauma will then be the cause of major lesions. As much as a 5 cm wound on the thigh does not have enormous consequences, as much a knife point inserted in the hand of barely a centimeter deep can cause great damage “.
What are hand pathologies?
Degenerative pathologies
The hand, like all the anatomy of the body, will undergo the signs of aging. It is the site of pathologies linked to cellular degeneration. We find :
- carpal tunnel syndrome
In addition to aging (promoting thickening of the tissues and in particular those of the tendons crossing the carpal tunnel), many pathologies generate carpal tunnel disorder. This is the case with diabetes, hypothyroidism, endocrine disorders…”We observe in the hand a compression of the median nerve which causes sensory disorders (paresthesia) at the level of the first three fingers of the hand. indicates the Professor. “At first the disorder is intermittent and then, if we do nothing, if we let the nerve be strangled day after day, the loss of sensitivity will set in..
Hand surgery can remedy this sensitivity, but it is not insignificant. “It is a surgery that can be a source of complications”, warn the doctor. “About 10 to 15% of operated patients do not instantly regain their sensitivity”. Before proposing the operation, the patient is suggested infiltrations. “An infiltration sometimes allows a woman to get through the peri-menopausal period and not be bothered afterwards”reassures the doctor.
- Trigger or spring fingers
Some people who try (often on waking) to stretch their palms and fingers, observe a blocking of one of the fingers followed by a sudden jump releasing the movement. “It’s a real embarrassment because the finger can remain blocked in a flexed position”recognizes the specialist.
The treatment initially consists in carrying out corticosteroid infiltrations in order to reduce the thickness of the synovium. If the infiltration is not effective or not possible, especially in the case of diabetes or if the finger is blocked in flexion, the operation is inevitable. “The procedure performed on an outpatient basis consists of opening the fibrous pulley that blocks the tendon”, describes the specialist. “Rehabilitation of the muscles and phalanges of the finger for a few weeks by the patient himself and his post-operative physiotherapist is necessary to avoid stiffening of the finger.
- osteoarthritis
On distingue :
- La rhizarthrose which corresponds to osteoarthritis of the trapezio-metacarpal joint. This is the base joint of the thumb. “Extremely well designed, this thumb joint over time will tend to operate in asymmetrical stress which will lead to the onset of osteoarthritis (especially in lax women), tells us the expert. Rhizarthrosis is symptomatic in 10% of women from 50 to 60 years old. It is therefore a common phenomenon but does not occur systematically. Only one in 10 is.. In some cases, the rhizarthrosis can also lodge between the metacarpus and the phalanx.
- Osteoarthritis in the other fingers is due to cartilage fragility often in a family context. It is common in the elderly and mainly affects the distal joints of the fingers (located between the second and third phalanges of the finger).
Surgery is not the first-line treatment for hand osteoarthritis.”We will first relieve people by applying local anti-inflammatories or by doing infiltrations”, offers the doctor. “For the thumb, if conservative treatments have failed, an operation is performed which consists of replacing the joint with a trapezio-metacarpal prosthesis. This is great because the patient is relieved quickly but the prosthesis wears out quickly. Thus, in younger patients, we can resect the joint and do ligamentoplasty, we are talking about trapezectomy”.
Before considering a surgical operation which would aim to set up a thumb prosthesis, it is possible to slow down the evolution of osteoarthritis of the thumb, thanks to exercises practiced regularly. The latter make it possible to optimize the resistance of the tendons of the trapezio-metacarpal zone and to soften the muscles. You can self-massage the palmar area, all the fingers and especially the area between the thumb and index finger. You will thus massage the muscles, the phalanges, the tendons (extensor, flexor), the ligaments in order to relax the whole of the hand. Do not hesitate to repeat these movements several times during the day. Intensify the back and forth movements on the area where the osteoarthritis is lodged. Do not hesitate to extend the movement towards the wrist for more comfort and relaxation.
Traumatic pathologies
- Fractures and sprains
They are relatively benign in the hand. We avoid as much as possible the operation in case of fractures because there is a risk of postoperative stiffness. “In the event of a traumatic accident on the flexor tendons (wound, knife blow, glass breakage), the operation remains inevitable because the tendon does not heal spontaneously and above all leads systematically, in the event of poorly carried out rehabilitation, to a loss of finger mobility (incomplete flexion and extension), would like to point out Professor Bertrand Coulet. Did you know that the scaphoid is one of the bones of the wrist (8 small bones form the carpus) most frequently fractured? It accounts for 60% of carpal bone fractures.
- Wounds
Due to the large number of vessels, tendons and nerves contained in a very small space that is the hand, all wounds of the hand, at the level of the fingers and the palmar region, must be explored in the operating room and preferably by a hand surgeon.
- Complex hand injuries
Very serious lesions of the fingers and the palmar region are classified by etiology: press hands (crushed hand), blast hands (fingers damaged by explosions of firecrackers), spinning top, pruning shears, car door hands ( grated hand between the road and the bodywork)… The treatment of lesions involves complex reconstructive surgery (in a high-level SOS hand centre). “It is important to find a center where the chain of care will be able to continue after the operation by having access to good care quickly (rehabilitation service with orthotist)”, advises Professor Bertrand Coulet. “In Europe and in Europe, the specialized centers are referenced within the European Federation of Main Emergency Services (FESUM)”.https://www.fesum.fr
Neurological syndromes causing paralysis
They include all the general pathologies that can…